- India
- International
Thursday, Apr 25, 2024
Journalism of Courage
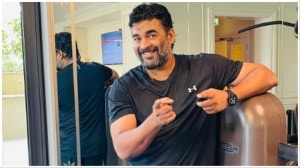
 AIIMS Director Dr Randeep Guleria with Senior Correspondent Kaunain Sheriff M at The Indian Express office. (Source: Express photo by Amit Mehra)
AIIMS Director Dr Randeep Guleria with Senior Correspondent Kaunain Sheriff M at The Indian Express office. (Source: Express photo by Amit Mehra)
The Director of All India Institute of Medical Sciences, Dr Randeep Guleria, talks about the need to return to the ‘family physician’ model, calls for “dramatic” change in medical curriculum and underlines the need for a single, “homogeneous” medical examination system at the state and national level
Why Randeep Guleria?
Appointed AIIMS Director in March this year, Dr Guleria joined the institution 23 years ago and is credited with setting up the country’s first pulmonology department. He is also the first Indian with a PhD in pulmonology and critical care medicine. During his tenure, AIIMS has conducted in-depth research on environment and its adverse effects on health. At a time when the Capital and many parts of North India are battling severe pollution, the AIIMS pulmonology centre is working on establishing a link between respiratory and cardiovascular diseases.
UNNI RAJEN SHANKER: How do we get back to the system of the general practitioner (GP)? Even when someone has fever, they are often confused about where or which GP to go to.
I agree. The concept of a family physician is disappearing, and in our country it is very important. In the West too, people are going back to the idea of a family doctor — as a first step — and then to a specialist. We are going the other way. The ‘general physician model’ is more European, where you have a structured plan. Your general physician refers you to a specialist; you cannot approach them directly. Here (in India), everyone wants to be a specialist. Not just in cities, even in rural India there is a huge need for general physicians. We are living in times where more and more doctors want to be specialists, instead of using their clinical skills. That needs to change.
ABANTIKA GHOSH: How important is clinical diagnosis? Does the fact that it is going out of fashion reveal a problem in the way we are teaching our doctors?

There is a need to overhaul the curriculum. It is not only how we are teaching our doctors, we must also look at how we can modify the curriculum to make it more, let’s say, student-friendly. Technology has changed so much, and we need to innovate as well. We need virtual teaching, more interaction with students and more case-based discussions. We need to find ways to get the student more interested in the subject instead of just relying on lectures. A lot of new things are happening in the field of medicine, they must become a part of the curriculum. So the curriculum has to change dramatically.
The curriculum has to evolve keeping in mind the changing technology and emerging diseases, or else no one will know what, say, Zika virus is. These emerging diseases such as Zika, Ebola etc need to find space in the curriculum.
 At a time when the Capital and many parts of North India are battling severe pollution, the AIIMS pulmonology centre is working on establishing a link between respiratory and cardiovascular diseases. (Source: Express photo by Amit Mehra)
At a time when the Capital and many parts of North India are battling severe pollution, the AIIMS pulmonology centre is working on establishing a link between respiratory and cardiovascular diseases. (Source: Express photo by Amit Mehra)
KAUNAIN SHERIFF M: You are a member of the Supreme Court-appointed advisory committee that is looking into the restructuring of the Medical Council of India (MCI). Have you spoken to the MCI? What has been the progress so far?
The committee has a bigger mandate, that of examining medical education in the country and finding ways to improve it. Ten years ago, there were more government medical colleges than private ones. Today, however, more than 60 per cent of MBBS or postgraduate seats are being offered by private colleges. What does this mean? In some places, the competitive examination process is not being followed; it is based on fees etc. So the quality of education is suffering. Then there are many colleges that have got approval but do not have enough infrastructure or faculty. I am not saying that we don’t need more doctors in the country — there is a huge shortage — but that should not be the reason for compromising on quality.
We could have a common exit exam for all students, irrespective of the college they pass out from. That could be one option, and there are many other things that we are looking at. So when we had an initial meeting of the oversight committee, that is one measure we discussed. The other important focus was on finding ways to improve the quality of education and the curriculum.
Also, with so many private colleges coming up, the number of seats has increased. Seats in government colleges have also increased. However, the infrastructure is not up to the mark. We have issues even in our institute (AIIMS), where we have more students now but the lecture theatre is small. It was never envisaged that the place will have so many students.
KAUNAIN SHERIFF M: Mental health is a big concern right now but psychiatry is still not taught as a separate subject but as a part of ‘general medicine’ in the MBBS curriculum.
When we start talking about curriculum, we also need to look at the time we have to complete the course. The curriculum is spread over five-and-a-half years; how are we going to accommodate everything into it? Are we going to increase the duration of the course or should we structure it differently?
You can either develop a programme where you cut some parts from the curriculum, add other things and then justify why you have done that, or you devise a system where, after a basic MBBS, you develop a soft module or training structure for the students. Let’s say you want to be a GP, then you get training to deal with issues of mental health etc. So, the development of curriculum has to be at a more local level.
Medicine has changed from what it was 30 years ago in terms of knowledge. And it is rapidly changing. I am fortunate that I am at AIIMS where there is exposure to the latest journals etc. But think of a physician in a smaller town who graduated from medical school 10 years ago. He is only dependent on what the medical representatives tell him, as far as knowledge is concerned. They will tell him about a new drug and claim that it is very useful. That doctor will then prescribe that drug without knowing if it is really needed. We need to develop a system of training and retraining our doctors so that they can stay in touch with the latest in healthcare.
 Appointed AIIMS Director in March this year, Dr Guleria joined the institution 23 years ago and is credited with setting up the country’s first pulmonology department. (Source: Express photo by Amit Mehra)
Appointed AIIMS Director in March this year, Dr Guleria joined the institution 23 years ago and is credited with setting up the country’s first pulmonology department. (Source: Express photo by Amit Mehra)
SHAILAJA BAJPAI: What do you make of the commercialisation of healthcare? While it has allowed more access — given the pressure on government hospitals — privatisation also has its drawbacks.
The fundamental question here is whether medicine is a service or a business. We need to take a call on that. Many of us first became doctors because we wanted to do service, not because we wanted to make money. The values have changed a lot, and medicine has paid a price for it. Medicine is a pure profession. A patient puts his life into your hands and you have the responsibility of being fair to that patient and doing the best that you can. But we are leaning towards the business model. Medical practice, medical education, patient care — now it is all about the money that you can make. We need to give these things some real thought.
UNNI RAJEN SHANKER: Is this because of the State abdicating its healthcare responsibilities…?
The State has to take responsibility for education and healthcare because the very fabric of the nation is dependent on it. We need more medical colleges with good infrastructure. We don’t need fancy private medical colleges, which are state-of-the-art but with no patients because they are unaffordable. We really need to rethink the entire process of medical education and patient care. The divide between corporate hospitals and the public sector is becoming huge. At government hospitals, not just at AIIMS, even in small towns, there are patients lying on the floor. They are not there by choice. These people can’t go to a private hospital because the cost is prohibitive. We have abandoned them in a way.
ABANTIKA GHOSH: The new AIIMS institutions are finding it hard to get faculty.
There are many reasons for people not joining the new AIIMS centres. For instance, the junior faculty want to join a nicely run hospital. I tell these people that they need to understand that when AIIMS was formed, the initial faculty was involved in structural design of the institution, rather than just patient care. It’s a process of evolution and doctors of the younger generation have to be a little more patient.
The second issue is the pay package, and the third is trying to meet the needs of doctors. People come to the hospital with expectations of a pathology lab, dialysis facility etc, and when they don’t get it, there is a sense of frustration. We need to look at how we can meet the needs of the faculty by talking to them. Paying them a lot of money is not the solution. I would argue that we need people who are dedicated to the profession irrespective of their salaries. They must work towards building the institute. AIIMS needs people who can toil and build the institution’s reputation or else it will become like any other general hospital.
KAUNAIN SHERIFF M: Do we need to rethink our medical entrance exams? Recently, questions have been raised about the National Eligibility Entrance Test (NEET), with people arguing that those with access to coaching centres and CBSE schools have a better chance of cracking the exam.
Yes, and not only medical entrance, but we need to look at the examination structures at different levels in the field of medicine. We have students who come in after their MBBS and don’t know how to put a urinary catheter. We need to move to a system of examination which looks at clinical skills instead of just theoretical knowledge.
MALLICA JOSHI: Is a common medical test the way forward?
In the long run, we will have to have one exam or else the system will become very complicated. I personally believe that there should be one examination and we should address the problems that are encountered by state board students. There should be a homogeneous system in place both at the state and the national level.
 During his tenure, AIIMS has conducted in-depth research on environment and its adverse effects on health. (Source: Express photo by Amit Mehra)
During his tenure, AIIMS has conducted in-depth research on environment and its adverse effects on health. (Source: Express photo by Amit Mehra)
RAHUL SABHARWAL: What kind of toll is the air in Delhi taking on its citizens?
We have been looking at it and it is a cause of concern. Pollution levels in Delhi have continued to be high for a long time. It is a silent killer. There is enough data from the Great London Smog (of 1952), from Los Angeles and various other parts of the world from the ’50s and ’60s — when they had a similar problem — to show that pollution causes significant morbidity and mortality.
Can I say for sure that a person died because of air pollution? I cannot. But it is a silent killer and a large number of people are affected by it. Look at what is being said by various cardiac associations, including the European Heart Association — they say that living in an area of high air pollution is as high a risk factor for heart attacks as is high cholesterol, high blood pressure or smoking.
We have studies that show that people who have high exposure to air pollution, their inflammatory markers are much higher, which makes them more susceptible to heart attacks later in life. So we need a multi-pronged approach to tackle it because it is bound to have long-term effects. There is a need to do something urgently.
Also, when we talk of pollution, we ignore indoor air pollution. Sixty per cent of India still uses biomass fuel for cooking — wood, cow dung etc. It is used in kitchens that are not properly ventilated. We need to find solutions for it too.
AAKASH JOSHI: In October, the Centre told the Supreme Court that it was vetting a draft law allowing passive euthanasia, but was opposed to permitting people to make a ‘living will’ — that they should not be put on life support in case of terminal illness — as it could be misused. How much do we need end of life care and what kind of legislation does it need?
It is an important issue and we need to have some policy on it. There are arguments in favour of decreasing suffering and looking at the quality of life rather than quantity of life, especially in patients who have terminal illness. There are people with terminal cancers, people who are critically ill and on ventilator support for days in the ICU with all those tubes inside them.
I think there needs to be a bigger debate on how to decrease the suffering of individuals who we know are terminally ill, and that is where euthanasia comes in. People say that it can get exploited, especially in cases where a large amount of property is involved etc. But if the individual has already issued a ‘living will’, stating that this is what he wants, then there should be some sort of a legal resort to strengthen the position of doctors in the situation.
 “I tell these people that they need to understand that when AIIMS was formed, the initial faculty was involved in structural design of the institution, rather than just patient care.” (Source: Express photo by Amit Mehra)
“I tell these people that they need to understand that when AIIMS was formed, the initial faculty was involved in structural design of the institution, rather than just patient care.” (Source: Express photo by Amit Mehra)
KAUNAIN SHERIFF M: How do we address the issue of lack of palliative care in our hospitals?
We are trying to make AIIMS a pain-free hospital. Not just for oncology, but the other departments as well (the cancer centre at AIIMS is pain-free). If we have nothing to offer people in terms of treatment, then at least we should try and reduce their suffering. We are developing programmes for palliative care. We are also looking at developing regular workshops and courses. I think we should offer better quality of life even if it is for a shorter duration.
KAUNAIN SHERIFF M: In April this year, the Prime Minister said that the government will bring a legal framework under which doctors will have to prescribe generic medicines which are cheaper than equivalent branded drugs. Do you think India is prepared to switch from commercial drugs to just generic ones? Are we ready for that kind of transformation?
I think it is important to understand the meaning of generic drugs. There are broadly three categories. One is the original drug, which is patented and made by the manufacturer — it is a ‘branded drug’. The second is the kind we have in India — the ‘branded generics’. Here, an India-based company makes use of the laxity in our patent laws and makes the same drug (branded) but under a different brand name. It is true for a number of companies — Ranbaxy, Cipla, Sun — all of them offer branded generics. The third drug is the ‘generic drug’, which does not have a brand, only the molecule’s name.
So the generic drug would be paracetamol, and Crocin or Calpol are the branded generics. So the branded generics, in a way, are also generics, but they are being promoted by an Indian company which makes it. The antibiotics made by the original company — one capsule or tablet — would be for, say, Rs 110. The branded generic made by Indian companies, however, will cost around Rs 15-20 and the generic drug will cost Rs 5 to 10. There is a huge difference in price.
The issue here is about quality control. The licence to make a product is either given by the DCGI (Drug Controller General of India) or the state DCGI. The DCGI argues that they don’t have enough inspectors to check all the sites. There is no quality control and so a lot of physicians are worried about generic drugs because they get made in facilities that may not be up to standards. Unless we are able to solve that problem — quality control for all generics — there will also be reluctance among doctors to use general generics. If we are able to ensure quality, then yes, these should be used. Also, there should be a system in place that instills confidence about the effectiveness of the drug.

JEE Main 2024 Session 2 Result: NTA has released the result for the April session of JEE Main 2024, with an increase in the number of 100 percentilers. Telangana has the highest number of toppers, followed by Maharashtra and Andhra Pradesh. However, states like West Bengal, Kerala, Madhya Pradesh, and Chhattisgarh did not have any 100 percentilers this year.